It is a proven fact that oral health has been associated with systemic conditions. Cardiac conditions have a direct interconnection with the oral cavity. People with oral disease are at higher risk for stroke, heart attack, and other cardiovascular conditions. Periodontal disease, vertical bone lesions, endodontic disease, dental caries, and dental infection were considered as dental conditions with some risk of entrapment in a relationship with cardiovascular disease (CVD).
1. Systemic Inflammation (Elevated CRP, IL-6, TNF-α)
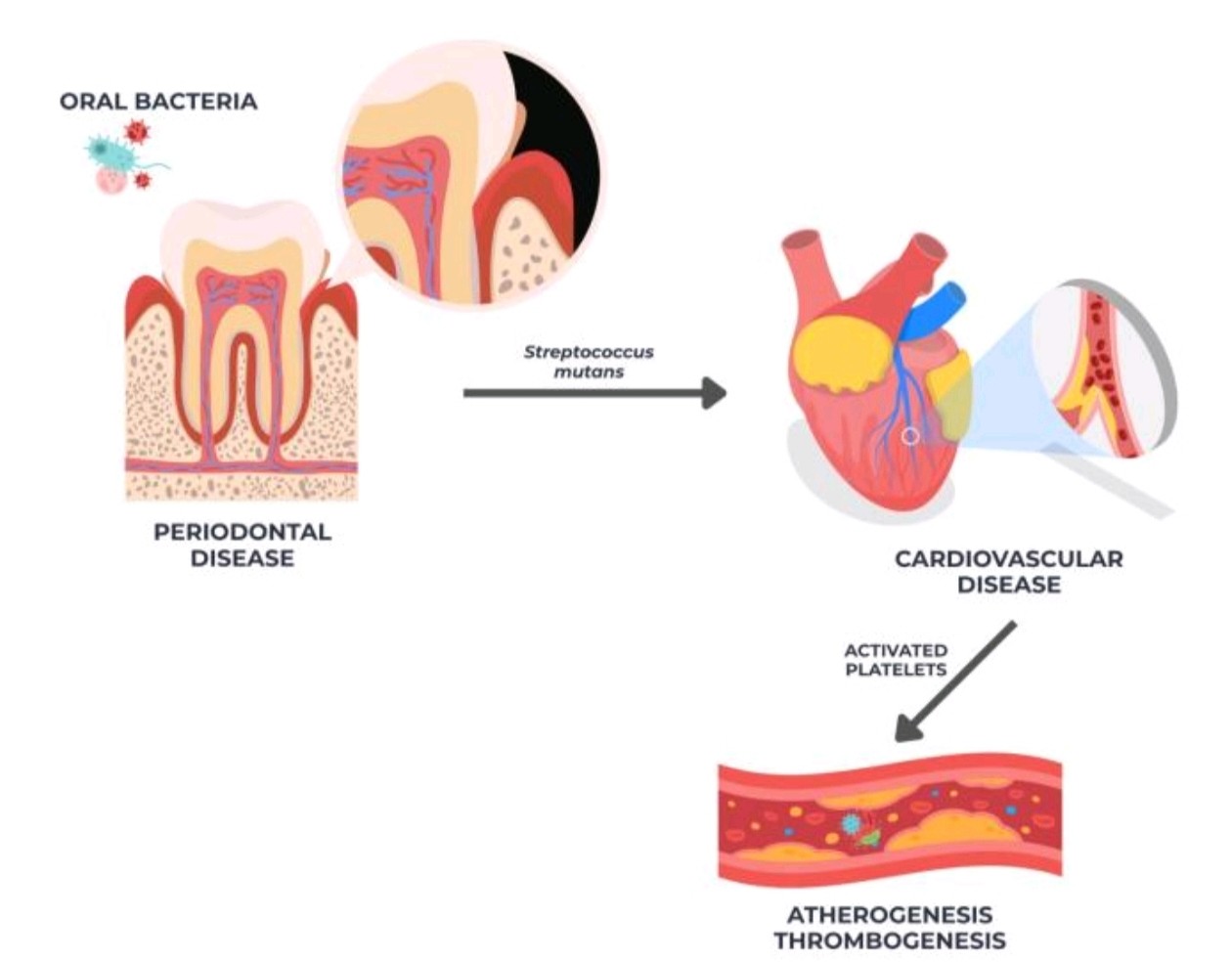
The mechanism between the oral-cardiovascular connection is due to systemic inflammation and microbial dissemination. The biological pathway is the sequential interaction between microbial invasion, immune activation, and vascular response.
The cascade is as follows:
Periodontal pathogens (Porphyromonas gingivalis, Aggregatibacter actinomycetemcomitans) → Reaches bloodstream → Release of cytokines → Promote endothelial activation, increased oxidative stress → Endothelial dysfunction and progressive arteriogenesis → Systemic inflammation
Oral bacteria (Streptococcus mutans and Streptococcus sanguinis) → Plaque activation → Thrombogenesis, inflammation, arteriogenesis, and localized thrombus formation
Inflammatory Cytokines
IL-6 → Promotes hepatic synthesis of C-Reactive Protein (CRP) and fibrinogen → Increases systemic inflammation and increased blood viscosity
TNF-α and IL-1β → Stimulate endothelial cells → Expresses adhesion molecules (VCAM-1 and ICAM-1) → Recruits circulating monocytes into intima → Differentiate into macrophages → Ingest oxidized lipoproteins → Forms foam cells → Initiates fatty streak development
CRP → Inhibition of endothelial nitric oxide (NO) synthase → Reduces NO bioavailability → Vasoconstriction and oxidative stress
CRP and high-sensitivity CRP can act as indicators of systemic inflammation.
2. Oral Microbiota in Atheromatous Tissue
Persistent oral infections could contribute to the pathogenesis of atherosclerosis. The periodontitis microbes could penetrate compromised oral mucosa such as ulcerated periodontal pockets to reach the bloodstream and reach other tissues. Evidence proves the presence of oral microbiome within cardiac atheromatous plaque.
The detection of Porphyromonas gingivalis DNA and LPS in atheromatous plaques supports the systemic translocation of bacterial products as a mechanistic link between oral dysbiosis and atherosclerosis
3. Xerostomia associated with antihypertensives
When patients take antihypertensive drugs such as Angiotensin-converting enzyme (ACE) inhibitors, calcium channel blockers, adrenergic blockers, and diuretics, they are more prone to decreased salivation. When salivation decreases, the chances of getting cavities, gum diseases, and candidiasis increase.
Treating the underlying salivary gland issues using biomedical engineering techniques, gene therapy, and stem cell therapy could help mitigate the issue.
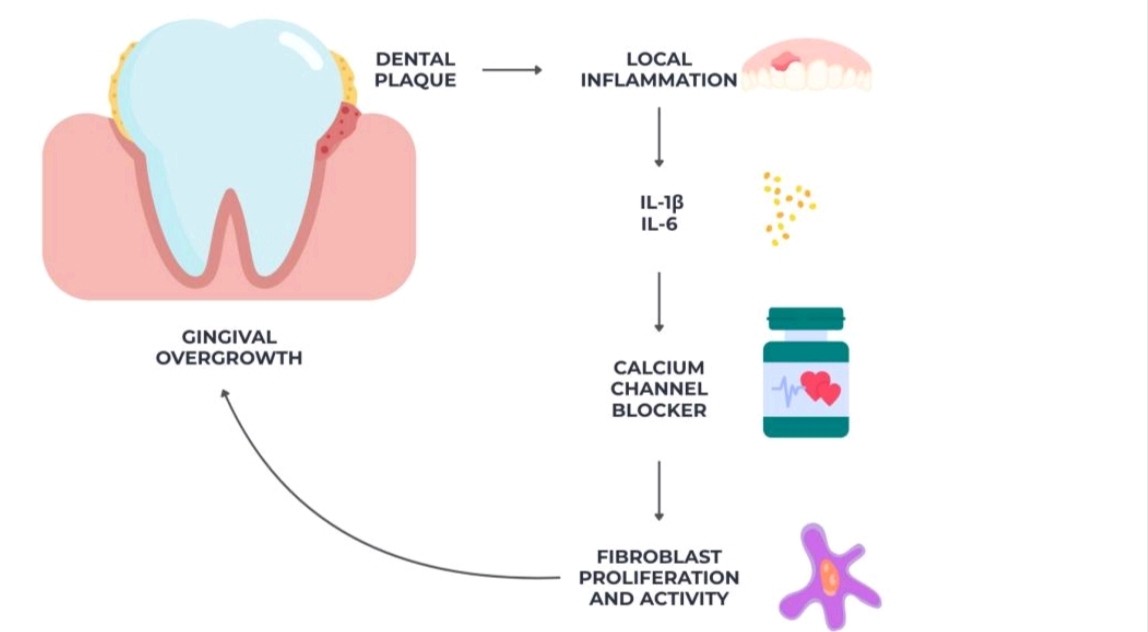
4. Gingival Overgrowth from Calcium Channel Blockers
Calcium channel blockers could increase the proliferation of fibroblasts, impair extracellular matrix breakdown, and reduce collagenase activity, leading to increased gingival growth. It deepens periodontal pockets and interferes with plaque control. It also favors the accumulation of anaerobic, periodontitis-associated bacteria such as Porphyromonas gingivalis and Prevotella intermedia, causing increased local inflammation and increased connective tissue destruction.
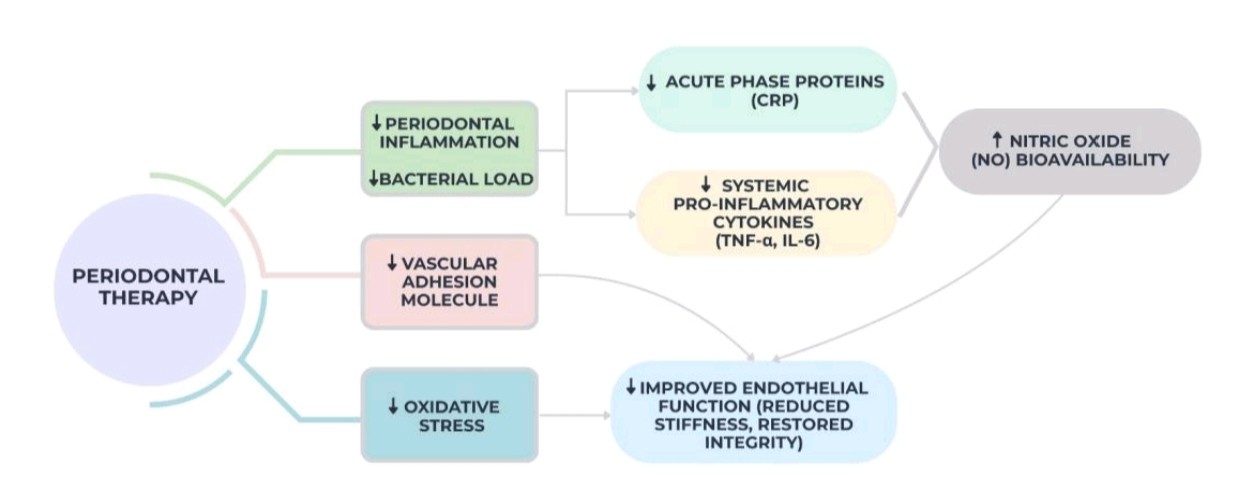
5. Improved Endothelial Function After Periodontal Therapy
After periodontal therapy in the form of scaling and root planing, evidence shows a reduction of systemic inflammation by reduction of cytokines, serum lipopolysaccharide, bacterial metabolites, such as short-chain fatty acids.
6. Oral Bleeding and Delayed Healing in Anticoagulated Patients
Oral bleeding is a clinically relevant complication frequently observed in patients undergoing long-term anticoagulant therapy, such as vitamin K antagonists (warfarin) or direct oral anticoagulants. Use of anticoagulants has also been linked to slower wound healing, which may be because these drugs interfere with fibrin production at the surgical site and change coagulation cascades.
7. Glossodynia and Burning Mouth in CVD Patients
Associations between cardiovascular disease, its pharmacological management, and burning oral symptoms have been suggested but remain poorly documented. Case reports describe burning sensations or glossodynia in patients treated with ACE inhibitors, supporting the hypothesis that certain antihypertensive medications may trigger secondary BMS.
8. Shared Risk Factors
Oral disease and CVD share common risk determinants such as smoking, diabetes, aging, and socioeconomic factors, which may act as confounders or effect modifiers in observed associations.
Key References
Association between Dental and Cardiovascular Diseases: A Systematic Review
Periodontal Disease and Cardiovascular Disease: Systemic Inflammation and Mechanistic Links
Periodontal Disease and Cardiovascular Disease Risk in Large Populations
Oral Hygiene and Systemic Health: Impact on Cardiovascular Risk
Umbrella Review of Periodontal and Cardiovascular Disease Association



